Droperidol: Everyone loves a Good Comeback Story

Brian Eby, MD, TLAF Fellow
For those starving for a non-COVID headline, I bring good news. Droperidol has returned to the US market after a two-decade hiatus. Banished from the US after its 2001 black box warning for deaths related to QT prolongation and torsades de pointes, droperidol was reintroduced here in 2019. Since then, it has been popping up on my hospitals’ formularies. As a junior physician with zero droperidol experience, I set out to familiarize myself with the Swiss Army Knife that is droperidol and share my findings below.
Similar to haloperidol, droperidol is part of the butyrophenone family of medications. It exerts its sedative effects by antagonizing the dopamine-2 receptor (D2-R), haloperidol’s main target. It was approved by the FDA in 1971 for nausea, vomiting, anxiety, and sedation. In the emergency department setting, it can be used for agitation, headaches, nausea, vomiting, and vertigo.
When it comes to agitated patients requiring chemical restraint, seconds count. Droperidol shines here as it has a rapid onset while also having a shorter duration than many sedatives. Both IM and IV dosing show onset in 3-10 minutes, peak in efficacy at 30 minutes, and wear off in 2-4 hours in most cases (1). Dosing for agitation is typically 5-10 mg IM. When compared to 10 mg haloperidol IM, 5 mg droperidol IM has been shown to be more effective and faster in onset when treating agitation in the ED (2, 3). When compared to 10 mg midazolam IM, 10 mg droperidol IM resulted in similar duration of violent behavior while requiring less additional doses of sedation and causing fewer cases of oversedation (4).
For nausea and vomiting, droperidol is an effective antiemetic in both the post-operative and emergent settings. Dosing for nausea is typically 1.25 mg droperidol IM or IV. This dose was shown to be more effective than 4 mg Zofran in the post-operative setting (5) as well as more effective than metoclopramide or prochlorperazine in the ED setting (6). However, the tradeoff may be a higher rate of akathisia, so it will not be my first line antiemetic (6).
As if that was not enough, droperidol is also a potent treatment for acute headaches. Both 2.5 mg IV and 5 mg IM have shown to ameliorate acute headaches better than prochlorperazine (7,8). A dose-ranging study pointed to 2.75 mg as the most efficacious dose for headache management while causing the least undesired effects (9). Thus, 2.5-2.75 mg is the dose I will reach for.
Finally, droperidol can also be considered for treatment of peripheral vertigo. Doses of 2.5 mg IM have been shown to relieve vertiginous symptoms in ED patients and are as effective as 50 mg dimenhydrinate (10, 11).
Okay, now what about the elephant in the room? The FDA released the black box warning in 2001 for an association of QT prolongation and torsade de pointes related deaths with droperidol. When this came out the potential legal ramifications of adverse events resulted in a near cessation of its use, its subsequent removal from formularies, and finally its removal from the US market. In hindsight, the data that triggered the black box warning appear suspect. Of the 277 cases of adverse events initially filed, there were actually only 65 individual cases (many duplicates) and, of them, only two of those were at doses commonly used in the US (12). The QT prolongation from droperidol is likely real, but dose dependent and minimal at doses used in the ED. Thus, it appears that droperidol is largely safe, but should be used with caution in patients that have known or suspected long QT.
Therefore, avoid using droperidol in males with QTc > 440 ms or females with QTc >450 ms, including those with congenital long QT. American Regent, maker of droperidol, recommends all patients receiving it should have an EKG (13), however this is unrealistic in the emergent setting. Before giving it, at least consider if the patient is at risk for long QT based on their known medications and past medication history. If you have any concerns, get an EKG or simply avoid droperidol. In addition, be mindful of other side effects such as oversedation, EPS such as dystonia and akathisia, NMS, and hypotension.
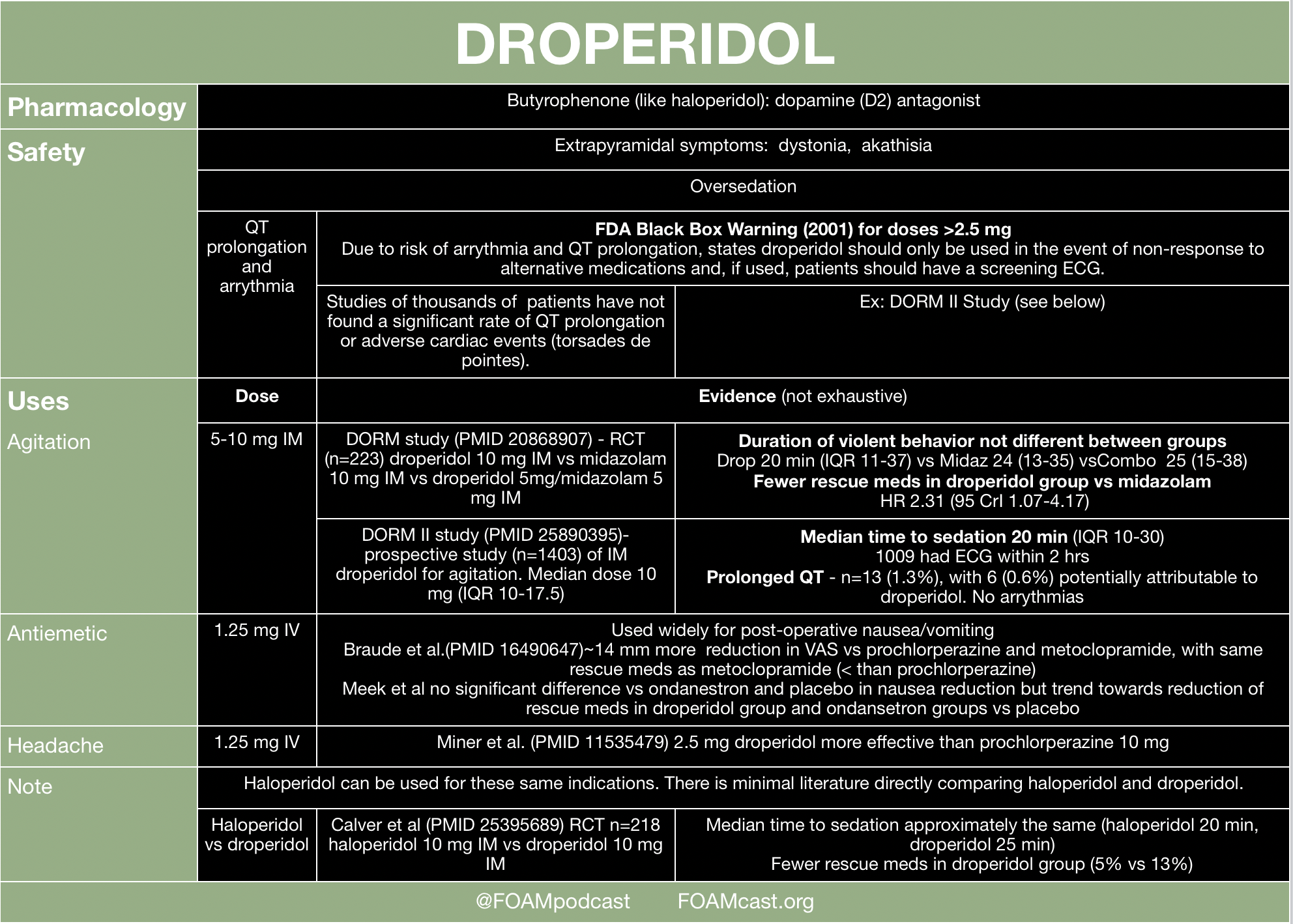
For a handy summary table (saved on my phone), please see foamcast.org’s image below.
https://foamcast.org/wp-content/uploads/2019/09/Screen-Shot-2019-09-02-at-6.51.14-AM.png
Full article https://foamcast.org/2019/09/02/droperidol-and-haloperidol/
For further reading, emDocs for a more in-depth review.
http://www.emdocs.net/droperidol-use-in-the-emergency-department-whats-old-is-new-again/
Brian Eby, MD
TLAF Fellow
Emergency Medicine Resident
UTSW/Parkland
[email protected]
References
1. Cressman WA, Plostnieks J, Johnson PC. Absorption, metabolism and excretion of droperidol by human subjects following intramuscular and intravenous administration. Anesthesiology. 1973;38:363-9.
2. Resnick M, Burton BT. Droperidol vs. haloperidol in the initial management of acutely agitated patients. J Clin Psychiatry. 1984;45:298-9.
3. Thomas H, Jr., Schwartz E, Petrilli R. Droperidol versus haloperidol for chemical restraint of agitated and combative patients. Ann Emerg Med. 1992;21:407-13.
4. Isbister GK, Calver LA, Page CB, Stokes B, Bryant JL, Downes MA. Randomized controlled trial of intramuscular droperidol versus midazolam for violence and acute behavioral disturbance: the DORM study. Ann Emerg Med. 2010;56:392-401 e1.
5. Fortney JT, Gan TJ, Graczyk S, et al. A comparison of the efficacy, safety, and patient satisfaction of ondansetron versus droperidol as antiemetics for elective outpatient surgical procedures. S3A-409 and S3A-410 Study Groups. Anesth Analg. 1998;86:731-8.
6. Braude D, Soliz T, Crandall C, Hendey G, Andrews J, Weichenthal L. Antiemetics in the ED: a randomized controlled trial comparing 3 common agents. Am J Emerg Med. 2006;24:177-82.
7. Weaver CS, Jones JB, Chisholm CD, et al. Droperidol vs prochlorperazine for the treatment of acute headache. J Emerg Med. 2004;26:145-50.
8. Miner JR, Fish SJ, Smith SW, Biros MH. Droperidol vs. prochlorperazine for benign headaches in the emergency department. Acad Emerg Med. 2001;8:873-9.
9 Silberstein SD, Young WB, Mendizabal JE, Rothrock JF, Alam AS. Acute migraine treatment with droperidol: A randomized, double-blind, placebo-controlled trial. Neurology. 2003;60:315-21.
10. Irving C, Richman PB, Kaiafas C, Eskin B, Ritter A, Allegra J. Droperidol for the treatment of acute peripheral vertigo. Am J Emerg Med. 1999;17:109-10.
11. Irving C, Richman P, Kaiafas C, Eskin B, Allegra J. Intramuscular droperidol versus intramuscular dimenhydrinate for the treatment of acute peripheral vertigo in the emergency department: a randomized clinical trial. Acad Emerg Med. 2002;9:650-3.
12. Jackson CW, Sheehan AH, Reddan JG. Evidence-based review of the black-box warning for droperidol. Am J Health Syst Pharm. 2007;64:1174-86
13. Kelly, G. American Regent Re-introduces Droperidol Injection, USP; AP Rated and Therapeutically Equivalent to Inapsine. American Regent Press Release. Feb 15 2019. <https://www.americanregent.com/media/2276/pp-dp-us-0011_droperidol_pressrelease_14feb2019.pdf>
|
{kind=link}